Transverse colon located appendix: A case of midgut malrotation
Midgut malrotation acut appendicitis
Authors
-
Yunus Kayci
Department of General Surgery, Adana State Hospital, Adana, Turkey
 https://orcid.org/0000-0001-8502-4367
https://orcid.org/0000-0001-8502-4367
-
Burak Yavuz
Department of General Surgery, Kozan State Hospital, Adana, Turkey
https://orcid.org/0000-0002-5262-0346
-
Ahmet Onur Demirel
Department of General Surgery, Kilis Prof. Dr. Aleaddin Yavaşça State Hospital, Kilis, Turkey
https://orcid.org/0000-0002-0313-5467
-
İbrahim Çoğal
Department of General Surgery, Çukurova University Medical Faculty Hospital, Adana, Turkey
https://orcid.org/0000-0002-4918-191X

Keywords:
acute appendicitis, atypical appendicitis, transverse colon, midgut malrotationAbstract
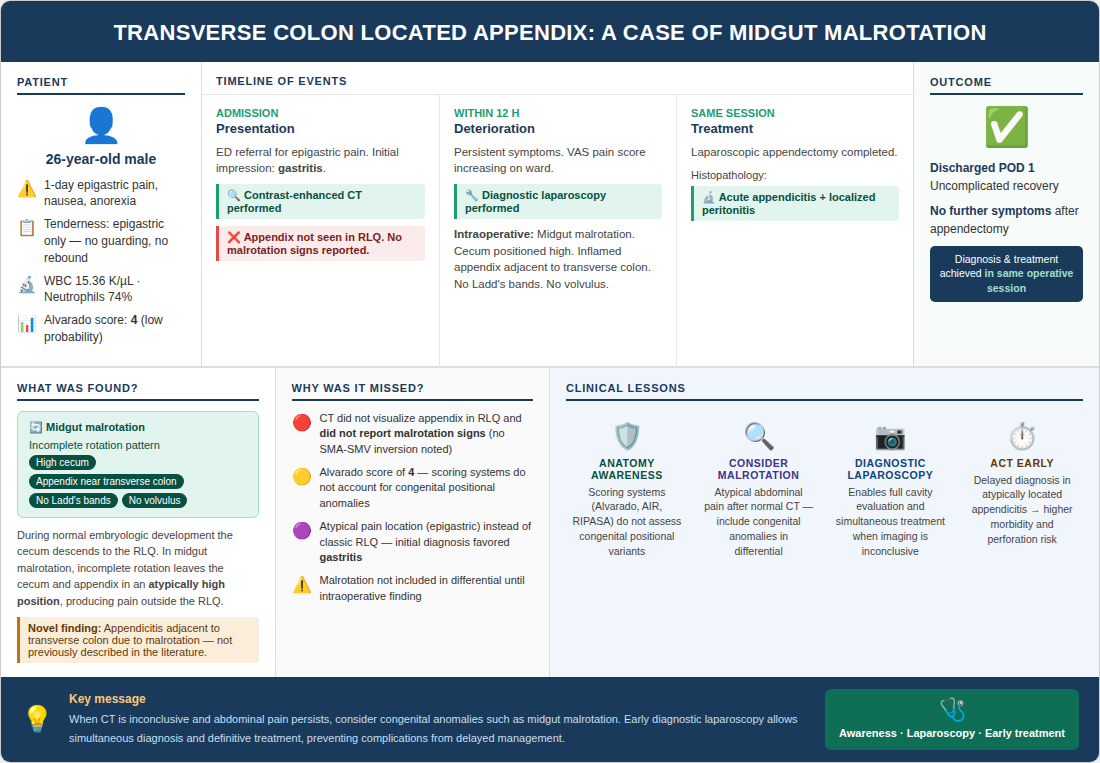
Acute appendicitis is the most common cause of abdominal pain requiring general surgical intervention in emergency departments. Its pathogenesis typically involves obstruction of the appendiceal lumen, followed by inflammation, ischemia, and potentially perforation or diffuse peritonitis. The Alvarado score is practical for bedside assessment; however, it does not account for anatomical variations of the vermiform appendix, which may delay diagnosis and increase complication rates. Midgut malrotation results from abnormal or incomplete rotation of the midgut during embryogenesis and may cause an atypically high position of the cecum and appendix. Appendicitis outside the right lower quadrant is associated with higher morbidity and mortality because clinical manifestations are variable and imaging may be inconclusive. We present a 26-year-old male patient admitted with one day of epigastric abdominal pain, nausea, and loss of appetite. Physical examination showed tenderness confined to the epigastrium, and laboratory evaluation revealed leukocytosis. Contrast-enhanced computed tomography did not visualize the appendix in the right lower quadrant and did not report signs suggestive of intestinal malrotation. Because symptoms persisted and pain increased during follow-up, diagnostic laparoscopy was performed within 12 hours of admission. Laparoscopy demonstrated midgut malrotation and an inflamed appendix located adjacent to the transverse colon; laparoscopic appendectomy was completed in the same session. The patient recovered uneventfully and was discharged 24 hours postoperatively, and histopathology confirmed acute appendicitis with localized peritonitis. Diagnostic laparoscopy is a valuable tool in atypical cases when clinical and radiological findings are insufficient, as it enables comprehensive evaluation of the abdominal cavity and allows definitive treatment without delay. In patients with atypical abdominal pain who cannot be diagnosed using conventional pathways, early consideration of congenital anomalies such as midgut malrotation and timely diagnostic laparoscopy are critical to prevent complications.
Downloads
References
Sakellariadis A, Sofou F, Chrysikos D, Sampsakos-Mariolis T, Schizas D, Troupis T, et al. Anatomical variations of the vermiform appendix. Acta Med Acad. 2024;53(3):335-42. doi: 10.5644/ama2006-124.461. DOI: https://doi.org/10.5644/ama2006-124.461
Rajasree G, Kumari MT, Chaganti G, Minz S. Anatomical deviations in the position of vermiform appendix: the cadaveric study. Siberian Scientific Medical Journal. 2022;42(3):36-40. doi: 10.18699/SSMJ20220303. DOI: https://doi.org/10.18699/SSMJ20220303
Lodhia J, Salewi AK, Sway H, Sadiq A, Msuya D. Late presentation of midgut malrotation in a young adult. J Surg Case Rep. 2022;2022(11):rjac515. doi: 10.1093/jscr/rjac515. DOI: https://doi.org/10.1093/jscr/rjac515
Patel RV, Jackson P, Zani A, De Coppi P. Laparoscopic management of midgut malrotation and tuberculous peritonitis in an adolescent boy. BMJ Case Rep. 2014;2014:bcr2013200714. doi: 10.1136/bcr-2013-200714. DOI: https://doi.org/10.1136/bcr-2013-200714
Miloudi N, Brahem M, Ben Abid S, Mzoughi Z, Arfa N, Khalfallah MT. Acute appendicitis in pregnancy: specific features of diagnosis and treatment. J Visc Surg. 2012;149(4):e275-9. doi: 10.1016/j.jviscsurg.2012.06.003. DOI: https://doi.org/10.1016/j.jviscsurg.2012.06.003
Mönttinen T, Kangaspunta H, Laukkarinen J, Ukkonen M. Nighttime appendectomy is safe and has similar outcomes as daytime appendectomy: a study of 1198 appendectomies. Scand J Surg. 2021;110(2):227-32. doi: 10.1177/1457496920938605. DOI: https://doi.org/10.1177/1457496920938605
Evola G, Ferrara F, Di Fede GF, Patanè M, Sarvà S, Piazza L. Left-sided acute appendicitis in a patient with situs viscerum inversus totalis: a case report. Int J Surg Case Rep. 2022;90:106658. doi: 10.1016/j.ijscr.2021.106658. DOI: https://doi.org/10.1016/j.ijscr.2021.106658
Shekhar A, Hendahewa R, Premaratne G. A diagnostic dilemma: left-sided appendicitis in a 10-year-old boy with previously undiagnosed intestinal malrotation. A case report. Int J Surg Case Rep. 2015;14:10-2. doi: 10.1016/j.ijscr.2015.06.036. DOI: https://doi.org/10.1016/j.ijscr.2015.06.036
Badak B. A rare cause of left lower quadrant abdominal pain: atypically located acute appendicitis due to malrotation: case report. Turk J Colorectal Dis. 2017;27:22-4. doi: 10.4274/tjcd.79106. DOI: https://doi.org/10.4274/tjcd.79106
Taslakian B, Issa G, Hourani R, Akel S. Left-sided appendicitis in children with congenital gastrointestinal malrotation: a diagnostic pitfall in the emergency department. BMJ Case Rep. 2013;2013:bcr2013009474. doi: 10.1136/bcr-2013-009474. DOI: https://doi.org/10.1136/bcr-2013-009474
Vagios I, Vailas M, Vergadis C, Schizas D. Transverse colon diverticulitis mimicking acute appendicitis. BMJ Case Rep. 2024;17(1):e254703. doi: 10.1136/bcr-2023-254703. DOI: https://doi.org/10.1136/bcr-2023-254703
Di Buono G, Buscemi S, Galia M, Maienza E, Amato G, Bonventre G, et al. Acute appendicitis and situs viscerum inversus: radiological and surgical approach-a systematic review. Eur J Med Res. 2023;28(1):85. doi: 10.1186/s40001-023-01059-w. DOI: https://doi.org/10.1186/s40001-023-01059-w
Krzyzak M, Mulrooney SM. Acute appendicitis review: background, epidemiology, diagnosis, and treatment. Cureus. 2020;12(6):e8562. doi: 10.7759/cureus.8562. DOI: https://doi.org/10.7759/cureus.8562
Chong CF, Adi MI, Thien A, Suyoi A, Mackie AJ, Tin AS, et al. Development of the RIPASA score: a new appendicitis scoring system for the diagnosis of acute appendicitis. Singapore Med J. 2010 Mar;51(3):220-5.
Downloads
- 155 171
Published
Issue
Section
How to Cite
License
Copyright (c) 2026 Yunus Kayci, Burak Yavuz, Ahmet Onur Demirel, İbrahim Çoğal

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Citations










